Deciding on which technique to use to treat our patients comes after careful consideration of examination, work-up and final diagnosis. Following this practice is essential when planning guided implant surgery. Utilizing the most appropriate plan is always the best and in situations where we place implants that are in close proximity to other vital anatomy; neurovascular structures, maxillary sinus and adjacent teeth or implants. Knowing and having a complete understanding of the precise location, exact dimensions and proximity of these structures to each other, means that the operator has a full three-dimensional depiction. Surgical dentistry requires precise skill and hand-eye coordination all within just millimeters. Working in an extremely small and micro-measured environment means we rely on specific tools to assist and guide our hands.
Indications for Guided Surgery:
· Reduce surgery time
· Tight surgical field with limited room
· Insure reproducible results
Guided Implant Surgery
I could make the argument for using guided surgery in all cases. My moto is “who wants to aim?”. Let’s be realistic we are treating people, some who have intense skepticism or fear of what they are about to experience. In order for us to rely on our “Spidey Senses” we need:
o A fully cooperative patient that maintains their head in the position we direct them into and we rely on them keeping their mouth open for the duration.
o Relaxed perioral musculature and tongue so that we can protect, manipulate and retract these tissues out of the field.
o To place a pharyngeal drape to prevent swallowing of or aspiration of a small dental tool.
o A dental assistant to suction fluids and materials to maintain a tidy surgical field. We rely on their ability to avoid getting in our way and maintaining the fluids within the oral cavity so patient isn’t filling up with irrigation requiring them to swallow.
Fully Guided Implant Surgery
Exactly like guided surgery with vertical control or height control. This type of surgery unlike guided surgery permits depth control for implant positioning. This means there is a hard stop that will not permit the twist drill past a preset depth, thus creating an exact three dimensional recreation of the precise position of the final implant fixture.



CASE REPORT
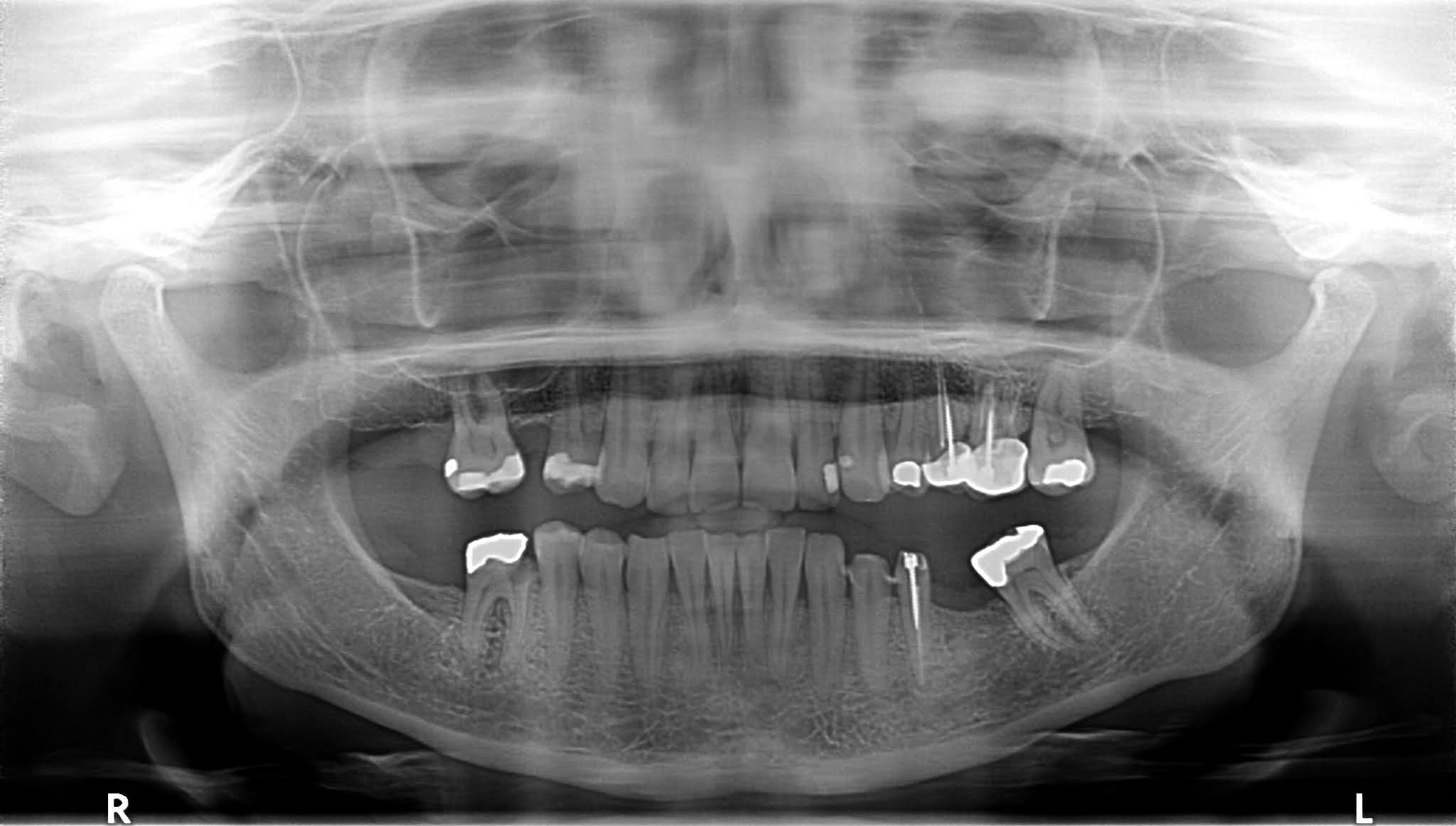
A 35 year old healthy woman presented emergently for extraction of a symptomatic non-restorable and advance caries, mandibular right first molar, #30. The patient requested restoration of her posterior occlusion after addressing her immediate problem. Tooth #30 was extracted and guided bone regeneration to preserve the alveolar ridge, was simultaneously performed with the addition of a xenograft and a resorbable collagen membrane over the socket. After uneventful post-op and four months, the patient returned for implant work-up for a CBCT of both arches and polyvinyl impression of the mandible. There is a guide fit test appointment and second review of the procedure and discussion of questions before the surgery and processing of pre-op prescriptions.
Surgical Guide Preparation
Utilizing implant planning software that melds the CBCT anatomy to the stone model or scanned data to create a computer-aided design and computer-aided manufacturing (CAD/CAM) stereolithographic (SLA) guides. See plan below.



Implant Surgery
Under moderated intravenous sedation non-restorable #18 was extracted first then using fully guided surgery which implies depth control, the universal surgi-guide and Simplant keys were used in succession from narrowest twist drill up to 4.3mm to accommodate this regular platform fixture. Position #19 4.3mm x 8mm and #30 4.3mm x 10mm were planned. Placement of short implants close to the mandibular neurovasculature may be a riskier procedure and a perfect indication for fully guided surgery. Surgery time 35 minutes.
Understand that placing implants using a surgical guide that rests on hard teeth versus soft tissue may have varying degrees of inaccuracies due to the nature of the base that the guide is supported.[1] Obviously soft tissue has a degree of mobility and can add inaccuracies versus hard tooth structure. Some research shows a larger average of 2.56mm of inaccuracy, with less in the maxilla, when placing implants within the mandible. In addition, using fully guided surgery in this system requires the use of just one guide versus three if placing a regular platform implant. The more we move and remove acrylic guides onto the arch, it can be a source of error if it’s not positioned perfectly. In addition, if during the procedure it is determined the fixture requires adjustment of its depth, it requires a work around.

The Girldoc😌
Comments